
Below The Knee Therapies
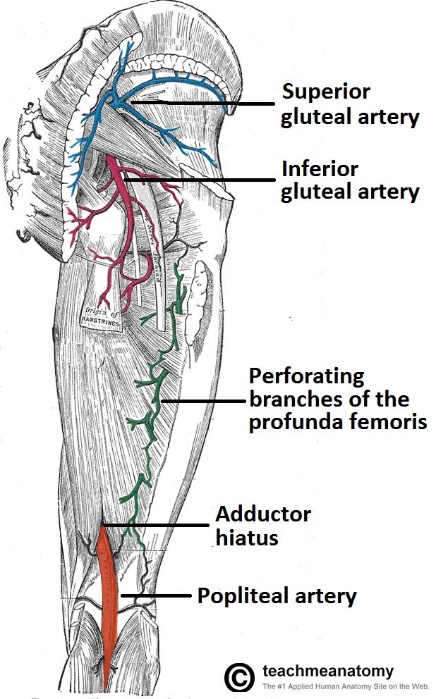
The popliteal artery descends down the posterior thigh, giving rise to genicular branches that supply the knee joint. It moves through the popliteal fossa, exiting between the gastrocnemius and popliteus muscles.
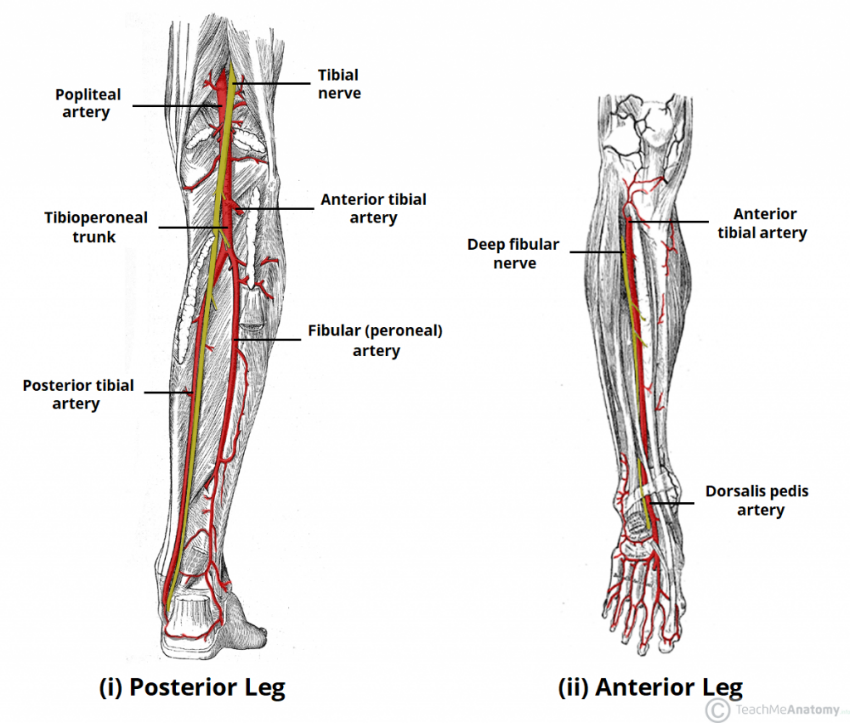
At the lower border of the popliteus, the popliteal artery terminates by dividing into the anterior tibial artery and the timiperone trunk. In turn, the timiperone trunk bifurcates into the posterior tibial and fibular arteries:
Posterior tibial artery – continues inferiorly, along the surface of the deep posterior leg muscles (such as tibialis posterior). It enters the sole of the foot via the tarsal tunnel, accompanying the tibial nerve.
Fibular (peroneal) artery – descends posteriorly to the fibula, within the posterior compartment of the leg. It gives rise to perforating branches, which penetrate the intermuscular septum to supply muscles in the lateral compartment of the leg.
The other division of the popliteal artery, the anterior tibial artery, passes anteriorly between the tibia and fibula, through a gap in the interosseous membrane. It then moves inferiorly down the leg. It runs down the entire length of the leg, and into the foot, where it becomes the dorsalis pedis artery.
Treatment of PAD includes lifestyle modifications—including smoking cessation and supervised exercise therapy—plus secondary prevention medications, including antiplatelet therapy, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, and statins.
Surgical or Endovascular revascularization should be considered for patients with lifestyle-limiting claudication who have an inadequate response to the aforementioned therapies. Patients with acute or limb-threatening limb ischemia should be referred immediately to a vascular specialist.